
By: Xinyu Zhang
Previous studies have well documented caregivers for older adults’ declined wellbeing. However, most studies use relatively less fine-grained measures that left the role of specific care activities in the daily lives unanswered. In a recent study published in The Gerontologist, SRC researcher Vicki Freedman and her colleagues used time diary data from the 2013 Disability and Use of Time (DUST) supplement to the Panel Study of Income Dynamics (PSID) to explore patterns of informal caregiving and experienced wellbeing over the day.
The measures in most studies of caregiving are not perfect. For example, respondents were typically asked to answer yes/no or to recall the number of hours in a typical week or month. These ways of measuring time spent on caregiving fail to capture precisely how time is spent on each task throughout the day. In addition, decontextualized wellbeing measures (e.g., ask respondents to recall their overall wellbeing over a reference period) cannot specifically evaluate the impact of caregiving.
Comparing to studies using aggregated measures of time use, the detailed diary data can capture both time use on specific tasks and momentary wellbeing. The diary interview asked about all activities happened on the previous day over a 24-hour period. The authors created ordered indicators of care for each 15-min interval. Caregiving activities were categorized as not care, household care, physical care, visiting/socializing, and transportation. To measure experienced wellbeing, respondents were asked to report how intensely they felt five emotions for up to three randomly selected diary activities.
The study found that caregivers on average spent 2.3 hours per day on caregiving, which is an hour less than global reports of care provided on the prior day with the DUST sample. One possible explanation of this result is social desirability effect; social pressure to over-report socially-favored activities relative to diary measure.
The researchers performed sequence and cluster analysis to characterize type and time of care activity. The result showed participation in care follows a roller-coaster pattern over the day, reaching peaks around mealtimes (10 a.m., 12p.m., and 5 p.m.). Five care types were identified with different intensities and activities. The authors found that 40% of caregivers provided only marginal assistance of about 1 hour per day and 28% provided sporadic assistance with a mix of activities for about 2 hours. Interestingly, marginal assistance providers reported lower experienced wellbeing than sporadic assistance providers. Their innovative work portrayed the patterns of older adults’ varying caregiving activities and further explored caregivers’ wellbeing.
Vicki Freedman, Jennifer Cornman, Deborah Carr, and Richard Lucas (2019). Time Use and Experienced Wellbeing of Older Caregivers: A Sequence Analysis. The Gerontologist.
Populations around the globe are aging at an astounding rate. Dementia, which primarily affects the elderly, and progressively impairs individuals’ abilities to think and perform everyday activities, is therefore also on the rise. According to the WHO, ‘[t]he number of people living with dementia worldwide is currently estimated at 47 million and is projected to increase to 75 million by 2030.’ Dementia imposes a high cost on both the individuals and families affected as well as on society in general.
In recent years, increased research interest has focused on dementia due to its rising toll. Researchers are interested in establishing quicker and more accurate diagnostic instruments for the primary care setting, and brief cognitive assessments also have high value for large studies of older adults. However, the brief cognitive assessments used for dementia classification are not perfect, yielding both false positives and false negatives which may impact care in clinical settings and findings in research settings.
In their recent article in Neurology: Clinical Practice, SRC researcher Kenneth Langa and co-authors analyze data from the population-based US Aging, Demographics and Memory Study (ADAMS) to determine predictors of dementia misclassification across three brief cognitive assessments. They examine clinical diagnoses from ADAMs as well as the implied diagnoses using the brief assessments, the Mini-Mental State Examination (MMSE), Memory Impairment Screen (MIS) and animal naming (AN).
All three brief assessments correctly diagnosed most individuals as having normal cognitive function or having dementia. However, false-positive and false-negative rates varied across the tests, and misclassifications were correlated with other factors, such as whether a relative or friend said the individual had a memory problem, age, education, illiteracy, race, and nursing home residency. Whether and to what extent each factor affected misclassification differed, however, among the three tests.
The researchers suggest that it could improve diagnostic accuracy to use different cutoffs on the brief cognitive assessments for individuals with different characteristics. Additionally, they point to an interesting finding that animal naming test achievement is negatively related to nursing home residency, possibly due to a tendency for lower verbal communication in residential facilities, or simply due to nursing home residents being quite ill; they recommend re-assessment after recovery.
World Health Organization, 10 Facts on Dementia. Accessed on 1/28/2019.
Ranson, Janice M., Elżbieta Kuźma, William Hamilton, Graciela Muniz-Terrera, Kenneth M. Langa, David J. Llewellyn. 2018. Predictors of dementia misclassification when using brief cognitive assessments. Neurology: Clinical Practice.
The prevalence of dementia in the United States is declining. But are all groups sharing in these gains? Earlier research found that there were large gaps in health between those living in urban versus rural areas, with the advantage going to urban dwellers. In a paper published recently in the American Journal of Preventive Medicine, SRC’s Ken Langa, with lead author Margaret Weden and co-authors Regina Shih from the RAND Corporation, and Mohammed Kabeto, used data from the Health and Retirement Study (HRS) to examine rural-urban gaps in cognitive health in a nationally representative sample for the first time.
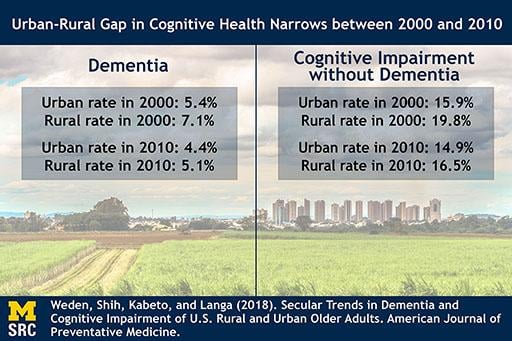
The HRS obtains information every two years on cognitive functioning that allows researchers to estimate the prevalence of dementia and what is known as cognitive impairment without dementia or CIND and changes over time. One way to look at urban-rural differences is to simply compare the rates of these health problems at two points in time. Langa and colleagues compared rural-urban differences in dementia and CIND in 2000 and then again in 2010. While both groups experienced declines in these problems, the declines were sharper for those living in rural areas, suggesting a narrowing of the rural-urban gap. The figure below shows that the prevalence of dementia in 2000 in urban areas was 5.4% in urban areas and 7.1% in rural areas. By 2010 those rates were 4.4% and 5.1% respectively. The pattern for CIND is similar.
This is very good news. But the story doesn’t end there. The researchers examined changes in sociodemographic characteristics of those living in rural and urban areas over that same period. Two major changes happened between 2000 and 2010. First, educational levels changed substantially in rural areas. In rural areas, between 2000 and 2010, the proportion of older adults with less than 12 years of education dropped by about half. This reflects the rapid increase and spread of high school graduation between 1910 and 1940. Second, the racial/ethnic composition of these areas changed as well. In particular, non-Hispanic blacks and Hispanics were a larger proportion of the population of urban areas than rural areas in 2010 than 2000. Interestingly, these changes account for much of the narrowing in the rural-urban gap in cognitive health. However, after taking into account sociodemographic and health factors there remained persisting rural disadvantages for dementia and CIND in 2000 and 2010. For example, the adjusted risk for dementia in 2010 was nearly 80% higher for rural compared to urban residents.
Margaret M. Weden, Regina A. Shih, Mohammed U. Kabeto, Kenneth M. Langa (2018). Secular Trends in Dementia and Cognitive Impairment of U.S. Rural and Urban Older Adults. American Journal of Preventative Medicine, 54(2): 164-172.

Delaying the age that retiring workers become eligible to receive the full amount of retirement benefit is an often-proposed solution to improve the financial stability of the Social Security system. Such proposal implicitly assumes that, on average, cohorts born later have higher life expectancy, so delaying the ‘full’ retirement age should not decrease the amount of lifetime benefit that these people eventually receive. However, in a paper recently published in Health Affairs, HwaJung Choi and SRC Professor Bob Schoeni showed that American workers born later are not in better health condition than the cohorts born earlier.
The original Social Security Act set the age for American workers to receive ‘full’ (unreduced) retirement benefits at 65. To reflect the increasing life expectancy, the 1983 Amendments set a gradual increase in the ‘full’ retirement age for people born after 1937. The increase was phased in over a 22-year period, eventually raised the full retirement age to 67 for people born in 1960 or later. Hence, according to the current rule, cohorts born later have to work up to two years longer before they are eligible to receive the full benefits than the cohorts born earlier.
Using data from the Health and Retirement Study (HRS) and the National Health Interview Survey (NHIS), Choi and Schoeni divided people born between 1933 and 1962 into four groups: those who are eligible to receive full retirement at age 65 (born 1933-1937), between 65 and 66 (born 1938-1942), at age 66 (born 1943-1954), between 66 and 67 (born 1955-1959), and at age 67 (born 1960-1962). They then examined several indicators of health conditions when each of these cohorts was at age 55-60. By comparing the health indicators at the same age across cohorts, they were able to show how health conditions have changed for each birth cohort in years leading to their respective retirement ages.
Choi and Schoeni found that, cohorts born more recently (and hence are only eligible to receive full Social Security benefit at ages higher than 65) are more likely to have limitations in their cognitive abilities and activities of daily living (ADL), as well as more likely to self-report as having fair or poor health, than the cohorts born earlier who can receive full benefit at age 65. When they split the sample by birth cohorts and levels of education, they also found that, holding the level of education constant, American workers who are eligible to receive full Social Security retirement benefit at later ages have higher morbidity of ADL limitations than those eligible to receive full benefit at age 65. The results regarding limitations in physical functioning and instrumental activities of daily living (IADL) are somewhat mixed; nevertheless, there is no evidence that the cohorts born later are in better health conditions than those born earlier.
Results reported by Choi and Schoeni are consistent with recent evidence that the health of near-elderly Americans has not improved in the past two decades. Given that people tend to claim retirement benefit at a later time as the full retirement age rises, the declining health conditions may lead to a higher share of workers in poor health conditions in the labor market. This would create challenges to employers and could potentially further destabilize the Social Security Disability Insurance (DI) program. Further increasing the full retirement age for the cohort approaching retirement may also cause substantial burden on these cohorts.
This article is published in Health Affairs:
HwaJung Choi and Robert F. Schoeni (2017). Health Of Americans Who Must Work Longer To Reach Social Security Retirement Age. Health Affairs, 36(10). https://doi.org/10.1377/hlthaff.2017.0217