
SRC researcher Margaret T. Hicken and collaborators recently published an analysis using Cox proportional hazards and linear mixed regression models to investigate residential neighborhood context and its relationship to chronic kidney disease (CKD), over time. The group published their findings in the American Journal of Kidney Diseases – the official journal of the National Kidney Foundation. Within five months of the publication of the article, news outlets have mentioned the article five times and social media has mentioned the article over three dozen times.
Context is an important factor in identifying risk for disease – specifically residential neighborhood. While lower neighborhood socioeconomic status and low access to healthy foods and spaces for physical activity have been associated with higher rates of hypertension, diabetes, and obesity, these factors have not been fully studied with respect to CKD risk. Furthermore, there are known disparities across race/ethnicity in prevalence of CKD and distribution of neighborhood contexts, with blacks experiencing higher levels of CKD, more neighborhood problems and worse neighborhood cohesion. Being able to identify features of the neighborhood beyond socioeconomic factors could help public health practitioners and clinicians identify important sources of stress and resilience may influence CKD-related health behaviors and thus help reduce these disparities.
These researchers capture aspects of residential neighborhood by creating scores based on participant-reported aspect of their neighborhoods at study entry for neighborhood problems (adequacy of food sources, availability of parks/playgrounds, noise, sidewalks, traffic, trash and litter, and violence) and social cohesion (attributes of people in their neighborhood including close knit, get along, willing to help neighbors, trustworthy, share values). They also examine kidney function in terms of an estimated glomerular filtration rate (eGFR; creatinine-cystatin C equation) and an indicator of eGFR decline (>30% across ten years and four exams).
The authors used baseline characteristics of participants in the Multi-Ethnic Study of Atherosclerosis (MESA) across quartiles of neighborhood problems and social cohesions scores. Next, they examined unadjusted cross-sectional associations between the neighborhood dimensions and eGFR at baseline. To examine the relationship between neighborhood dimensions and eGFR decline over time, they used linear mixed models with random intercepts, accounting for the correlation within participants. In addition to their unadjusted model, they build a second set of epidemiological models by including individual-level sociodemographic factors and MESA study site as confounders and then a third model including potential mediators that may link neighborhood context to eGFR decline in a fully specified model.
The authors report no association between the neighborhood scores and eGFR in the baseline models within any of the race/ethnic groups. In the longitudinal analyses, the hazard of an eGFR decline >30% from baseline was not statistically different for those in the highest quartile of neighborhood problems to the lowest quartile, though the decline in eGFR for those with greater neighborhood problems was greater than for those in the lowest quartile of problems.
At the conclusion, the authors state their null findings may be interpreted in several ways. It is possible that perceived social environment does not play an important role in very early stages of CKD. Null findings could have been a result of measurement error, as neighborhood social context is difficult to measure without error. Social context may be interrelated with neighborhood sociodemographic characteristics and disentangling the two may be difficult. They also note that individual-level factors (e.g. individual-level SES) may be important with eGFR decline in a healthy cohort – though literature on this topic is unclear.
Despite the null findings of this study, neighborhood SES has been a consistently associated with known risk factors for CKD including incident hypertension, cardiovascular disease, diabetes, and smoking prevalence, inflammatory markers, depressive symptoms, and alcohol use. With the large disparities in CKD and in neighborhood context between blacks and whites, combined with the null findings in these race/ethnic groups between CKD and neighborhood context, the authors suggest that future work should examine the role of racial residential segregation.
In order to uncover the origins of these pronounced health disparities (e.g. CKD); we need to have a clear picture of what is, and what is not. I feel it is extremely important to publish these null findings, and appreciate that the authors, and the journal, have taken the time to carefully lay out their analysis and publish the results – even as null results.
Hicken, Margaret T., Ronit Katz, Carmen A. Peralta, Deidra C. Crews, and Holly J. Kramer. 2019. ‘Neighborhood Social Context and Kidney Function Over Time: The Multi-Ethnic Study of Atherosclerosis‘ American Journal of Kidney Diseases 73 (5): 585-95.

A large set of research literature has shown that religiosity is associated with better health. The association can be attributed to several reasons: religious activities may promote social support, healthy lifestyles, and other psychosocial factors associated with better life outcomes.
In two recent papers, one published in the Journals of Gerontology: Social Sciences and the other in SSM Population Health, SRC researcher Mary Beth Ofstedal and her colleagues show that religiosity improves life expectancy in the U.S. They also show that the association between religiosity and health varies across countries with different social institutions around the world.
In the first study, they use the Health and Retirement Study to examine the effect of religiosity (measured in attitudes toward religion and religious service attendance) on life expectancy. In particular, because disability has an adverse effect on life quality, they also split total life expectancy (LE) into disability-free LE and disabled LE.
Distinguishing disability-free LE vs. disabled LE is an important contribution to the literature. While an increase in LE is favorable, it is even more so when it is accompanied by increases in disability-free rather than disabled LE. Ofstedal and colleagues show that, in the U.S. context, both positive attitudes toward religion and higher levels of participation are associated with improved LE, and most of the increase in LE is in the form of additional disability-free years. On average, a higher level of religiosity improves LE for near-elderly women more than men.
In the second study, the World Values Survey, which consists of data from 93 countries, is used to study whether the relationships between various measures of religiosity and health hold across different countries in a global context. Three measures of religiosity are utilized: participation (frequency of religious activity attendance), importance (the importance of god in one’s life), and meaning (frequency that one ponders the purpose of life).
Ofstedal and her colleagues show that the relationship between religiosity and health varies across countries. For example, although participation is positively associated with health on average, the association is positive in some countries but negative in others. The relationship between importance/meaning and health also demonstrates substantial variation across countries. Furthermore, within the same country, the relationship often flips signs when one measure of religiosity is used versus another. Only three countries exhibit positive relationships between all three measures of religiosity and health.
To explore this variation in effects further, several indicators at the country level are introduced: country-level religious diversity, the country’s restriction on religion, the country’s human development index (HDI), and whether a country is or has been governed with communism. Results suggest that participation is more likely to be associated with better health in countries where there is a higher degree of diversity in religion. On the other hand, importance and meaning of religion is more likely positively associated with health in countries where there is a higher level of restriction on religion and/or a lower HDI. The relationship between religiosity and health is also more negative in current or former communist countries.
The authors speculate upon the reasons that lead to the variations in effect size across countries and measures. They argue that participation in religious activities is more likely to improve health where participation is voluntary. In countries where participation is not as voluntary, the salutary effect on health might be suppressed. Furthermore, in less developed countries (lower HDI) or where religion is constrained, stronger belief is more likely to be beneficial and hence improve otherwise difficult lives.
Mary Beth Ofstedal, Chi-Tsun Chiu, Carol Jagger, Yasuhiko Saito, Zachary Zimmer (2018). Religion, Life Expectancy, and Disability-Free Life Expectancy Among Older Women and Men in the United States. Journals of Gerontology: Social Sciences.
Zachary Zimmer, Florencia Rojo, Mary Beth Ofstedal, Chi-Tsun Chiu, Yasuhiko Saito, Carol Jagger (2019). Religiosity and health: A global comparative study. SSM – Population Health, 7: 100322.
Transgender adults’ daily lives are filled with discrimination, worry, anxiety, and actions taken to brace for discrimination, according to a survey of 316 transgender-gender non-conforming (TGNC) U.S. adults led by Transcend the Binary, a transgender advocacy organization in Ferndale, Michigan with assistance from U-M researchers. The TGNC community shows resiliency through its efforts to advocate for individual gender identity recognition and respect, and its strong within-community support systems.
The survey, Finding our Strength, was a community-led effort in determining its research objectives, questionnaire development, analysis and sharing of results. ‘A community-led process was essential to ensure that the survey was responsive to community needs, gender-affirming, and supported by the community,’ said ISR researcher, Peter Batra responsible for the survey data analysis. Transcend the Binary assembled a core research team, identified TGNC community members for focus group participation, and brought forward scores of individuals to assist with the survey development and data interpretation. ‘A community-led process creates synergy by building on trust, learning through shared experiences, skill sharing and collaborative decision making’ explains Transcend the Binary co-founder and Executive Director, Brayden Misiolek.
This community-led process was evident in the manner in which gender identity data was collected. ‘Transcend the Binary is adamant that gender identity is defined by the individual and that respect must be given to each person’s authentic gender,’ stated Misiolek. Thus, gender identity was asked through an open-ended question. This resulted in over 120 unique gender identities being reported: a perfect illustration that gender identity lies across a spectrum that goes far beyond the binary. Survey respondents reported that they identified as TGNC at an average age of 18 years and were open to others about their gender at an average age of 20. However, the age range at which these events occurred varied greatly with older respondents being more likely to have waited decades before revealing their authentic gender identity to others.
Since there is no national sampling frame available for the TGNC community, the survey relied on a convenience or snowball’ recruitment method for participants. Transcend the Binary led the recruitment process through community outreach and social media messaging. This yielded a population that was typically less than 30 years old, white, had at least some college education and reported a low household annual income. These population characteristics were similar to the participant characteristics of the U.S. National Transgender Survey (2015).
A major survey finding was the high percentage of participants that reported anxiety. Using the General Anxiety Disorder-7 scale, four of five respondents reported some degree of anxiety with over 30% reporting severe anxiety. ‘This level of anxiety is higher than that reported in the literature, but was felt to be a valid finding by our local TGNC community,’ said Caitlin Tupper, LCSW, of Transcend. ‘Among our respondents higher anxiety was associated with less family support, lower self-reported health status and coping through avoidance or social isolation.’

The survey expanded the information about experienced discrimination reported in the U.S. National Transgender Survey by focusing on discrimination worry and actions taken in anticipation of discrimination (i.e., hypervigilance). Ninety-eight percent of respondents reported worrying about discrimination in personal or social situations at home or at family or social gatherings. Discrimination was also present in healthcare settings. About half (55%) of respondents worried about discrimination from primary care providers, while 42% and 60% worried about discrimination from pharmacists and psychiatrists, respectively. Only 12% worried about discrimination when seeing a transgender specialists. ‘The results indicate that education about transgender health and gender-affirming care can help to lower discrimination worry,’ says Misiolek.
A key component of community-led research is sharing the information not only with the TGNC community but with the wider public along with translating survey findings into action. Transcend the Binary has led such an effort via multiple initiatives including an interactive art exhibit of the findings, educational programs for health practitioners, students, and at public health and transgender health conferences, and general public presentations like the one held at ISR in November 2018. It has also used its findings to inform its own client advocacy and support work.
‘Our research is just a glimpse into the lives of the TGNC community,’ says Nancy JW Lewis, PharmD, MPH a U-M co-investigator. ‘Ways to bring the voices of those most marginalized within the community, including persons of color and the elderly, into future research is needed.’
Information about Transcend the Binary is available at www.transcendthebinary.org, along with a report of more detailed survey results: http://www.transcendthebinary.org/wp-content/uploads/2017/12/Finding-Our-Strength-Survey-Report.pdf
By: Brooke Helppie-McFall and Taylor Slayton
Losing money is difficult for everyone, but new research by Lindsay Pool, Sarah Burgard, Belinda Needham, Michael Elliott, Kenneth Langa, and Carlos Mendes de Leon in the Journal of the American Medical Association in April, 2018 show that suffering a negative wealth shock may even increase risk of death.
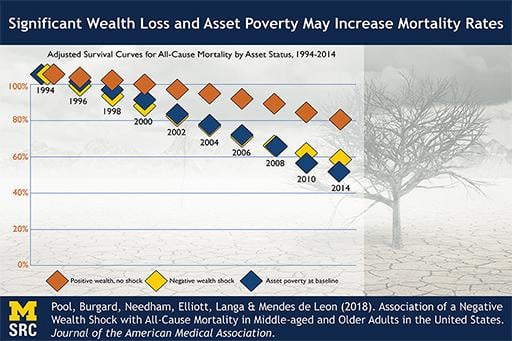
Research has previously linked loss of wealth to short-term health changes such as increased risk of depression and anxiety, substance abuse, and suicide. Pool and co-authors use data from the Health and Retirement Study (HRS) to study the long-term effects of negative wealth shocks on all-cause mortality rates. They examine the link between suffering a negative wealth shock (defined as a wealth loss of 75% or more between 1992 and 1994) or asset poverty (having zero or negative wealth in 1992), and the total all-cause mortality rate over the twenty years beginning in 1994. The study sample included adults in the United States who were born between 1931 and 1941.
In the study sample, 26.2% of people experienced a negative wealth shock and 6.9% had asset poverty between 1992 and 1994. Those who experienced a negative wealth shock or asset poverty were more likely to be women, non-white, have lower levels of household income and net worth, and be in poor health relative those who did not.
Compared to a similar person who did not experience a shock or asset poverty, the researchers found that a person who experienced a negative wealth shock had a 50% higher risk of mortality during the following 20 years, and a person with asset poverty at the beginning of the period had a 67% higher risk of mortality over that same 20-year period. Wealth shocks in which older adults lose their primary place of residence resulted in an even higher increase in mortality risk. The researchers discussed possible pathways for these associations. They stated that the stress of economic loss in one’s 50s or 60s may contribute to a higher risk of mental health conditions or substance abuse, which in turn may result in a long term increased risk of mortality, especially combined with the inability to pay for treatment. Additionally, stress due to wealth loss may cause short-term increases in blood pressure or inflammation, increasing risk of cardiovascular mortality. Indeed, their findings are consistent with all of these stories.
The authors note that the passing of the Affordable Care Act (ACA) appears to have a mitigating effect on the impact of wealth shocks on mortality, since it has reduced the prevalence of negative wealth shocks caused by medical issues. This issue will be one to watch after more post-ACA data become available in the coming years.
Pool, Burgard, Needham, Elliott, Langa & Mendes de Leon (2018). Association of a Negative Wealth Shock with All-Cause Mortality in Middle-aged and Older Adults in the United States. Journal of the American Medical Association.
The frequent occurrence of sexual assaults on college campuses has focused national attention on this important public health concern, with estimates of sexual assault rates as high as 20% reported for undergraduate women. However, an important knowledge gap exists regarding rates of sexual assault for young adults in general, in that accurate population-based prevalence rates for both women and men who do and do not attend college are not readily available.
In a recent study, SRC Research Professor William Axinn, SRC Research Associate Professor Brady West, and recent MPSM Graduate Maura Bardos aimed to address this knowledge gap by characterizing rates of forced sexual intercourse for individuals with different amounts of college education. Forced intercourse is an important subset of total sexual assaults that represents nearly half of all sexual assaults. Axinn and colleagues accounted for age and college attendance in their analyses and characterized types of force experienced with forced sexual intercourse. To derive population-based estimates for forced sexual intercourse, Axinn and colleagues utilized data from the U.S. National Survey of Family Growth (NSFG), which offers a nationally representative sample of approximately 5,000 U.S. women and men ages 15 – 44. Two cohorts (2002 and 2011-13) were included in this study to assess prevalence rates over time. The NSFG study focuses on family life, reproductive health, marriage and divorce. Methodologically, the NSFG is designed to reduce reporting bias by utilizing audio-computer assisted self-interviewing (ACASI) to provide privacy and immediate encryption about sensitive information.
Axinn and colleagues estimated that approximately 20% of U.S. women aged 18-44 have ever been forced to have vaginal intercourse, which is similar to rates of sexual assault reported in college campus populations. Estimates of forced sexual assault increased with age, which may reflect increased exposure to risk with time. By the age of 44, approximately one in four women reported an experience of forced sexual intercourse, according to the study estimates. Lifetime estimates were generally lower for men, with approximately 6.5% reporting ever having experienced forced sexual intercourse. Unlike the monotonic increase in assaults associated with age in women, the rates changed in both directions across age groups for men. In the decade between the two NSFG cohorts, rates remained relatively stable for both women and men.
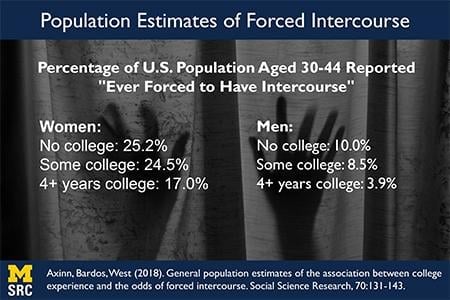
Women and men with four or more years of college reported lower rates of forced sexual intercourse. Women with fewer than four years of college education had 2.5 times higher odds of ever experiencing forced sexual intercourse then individuals with four or more years of college. For men with less than four years of college, the odds of ever experiencing forced sexual intercourse were 4 times higher compared to men with four or more years of college education. These findings generally held when adjusting for covariates associated with selection into college education. For both women and men, verbal pressure or abuse was the most frequently cited type of force experienced during the sexual assault.
The estimated rates of forced sexual intercourse highlight that sexual assault is a clear public health concern for both women and men, and in the decade between NSFG assessments there is no evidence of a decline in prevalence. It should also be noted that total sexual assault rates in the population are likely higher than reported here, because NSFG estimates are based on lifetime experiences and reflect only one subtype type of sexual assault. This underscores the need for more research to further characterize the full range of sexual assaults and associated consequences. Given that the majority of U.S. adults do not complete four or more years of college education, it is critical to expand intervention research to consider the unique contextual factors associated with individuals not attending college since these adults are at the highest risk for experiencing sexual assault.
William Axinn, Maura Bardos, Brady West (2018). General population estimates of the association between college experience and the odds of forced intercourse. Social Science Research, 70:131-143.
In a recent paper published in the International Journal of Epidemiology, SRC research assistant professor Hongwei Xu and his colleagues studied how early-life exposure to China’s 1959-1961 famine affected cognitive performance in midlife. They found some support that nutritional deprivation during prenatal and early postnatal periods had negative impact on both the level and the change of cognitive performance among Chinese adults in their 50s.
In theory, malnutrition during prenatal and early postnatal period due to exposure to famine may alter the process of brain development, which negatively affects cognitive ability. Such negative effects on cognitive ability can also have a latent period and will only show up in the mid- to old- ages. However, results from previous research based on the 1944-1945 Dutch famine did not support such argument.
The Chinese famine that began in 1959 and ended in 1961 were largely attributed to both natural disasters as well as policy mistakes after the onset of Great Leap Forward (GLF) campaign in 1958 (hence the ‘GLF famine’). Compared to other famines, the GLF famine lasted longer, had a wider geographic scope, and caused a greater death toll. Hence, if prenatal and early life exposure to malnutrition did have adverse effects on cognitive ability, the effect would be more pronounced in the case of the GLF famine.
Hongwei and his colleagues reexamined this question using data from the China Health and Retirement Longitudinal Study (CHARLS), a nationally-representative survey of Chinese adults who are aged 45 or older. Samples from multiple cohorts born between 1958 and 1963 in various geographic locations were used, and these cohorts varied in timing, duration, and intensity of exposure to the famine.
In particular, people who were born between 1958 and 1963 were exposed to the famine and hence malnutrition in various ways: between birth and year of age three for the 1958 cohort, between in utero and year of age two for the 1959 cohort, between in utero and year of age one for the 1960 cohort, etc. The 1963 cohort, who were not exposed to the GLF famine (including pre- and postnatal periods), were used as a control group.
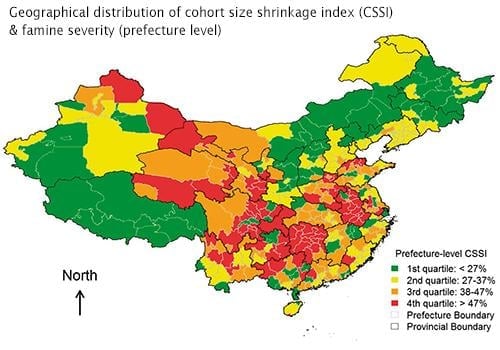
The severity of famine was measured at the prefecture level (the famine hit rural areas harder) and was defined as the difference in mortality between the famine period and the years immediately before/after the famine period. Two waves (2011 and 2013) of the CHARLS data were used, so the researchers could examine the effect of famine on not only the level of mid-life cognitive performance in 2011 but also the change of mid-life cognitive performance between 2011 and 2013.
Overall, Hongwei and his colleagues found some, but somewhat limited, support that exposure to famine negatively affected cognition. First, comparing to the 1963 cohort (the control group), the 1961 cohort had lower score in cognitive performance in their mid-lives. Nevertheless, no other cohort born between 1958 and 1962 demonstrated different cognitive score from the control group. Second, the 1959 cohort, who arguably were most adversely affected by the famine, were the only cohort that experienced statistically significant decline in cognitive ability between 2011 and 2013.
One plausible explanation to their mixed results is the mortality selection effect. To the extent that the 1958-1961 cohorts were hit the most during the famine, many of them may not have survived long enough to be surveyed in 2011. In other words, people who were hit the most but managed to survive into their 50s were a very selective (i.e. ‘tougher’) subsample of their birth cohort. Consequently, even though on average famine negatively affected cognitive performance, such effect might not be observed among the ‘tougher’ surviving subsample. However, the negative impact on cognitive decline still exists. This explains why the negative effect of famine on the level of cognitive ability was only observed in the younger cohort (who were not hit as hard) as well as why the negative effect of famine on the change in cognitive ability was only observed among the 1959 cohort (who were hit the hardest).
Hongwei Xu, Zhenmei Zhang, Lydia Li, Jinyu Liu (2018). Early life exposure to China’s 1959-61 famine and midlife cognition. International Journal of Epidemiology, 47(1): 109-120.

Delaying the age that retiring workers become eligible to receive the full amount of retirement benefit is an often-proposed solution to improve the financial stability of the Social Security system. Such proposal implicitly assumes that, on average, cohorts born later have higher life expectancy, so delaying the ‘full’ retirement age should not decrease the amount of lifetime benefit that these people eventually receive. However, in a paper recently published in Health Affairs, HwaJung Choi and SRC Professor Bob Schoeni showed that American workers born later are not in better health condition than the cohorts born earlier.
The original Social Security Act set the age for American workers to receive ‘full’ (unreduced) retirement benefits at 65. To reflect the increasing life expectancy, the 1983 Amendments set a gradual increase in the ‘full’ retirement age for people born after 1937. The increase was phased in over a 22-year period, eventually raised the full retirement age to 67 for people born in 1960 or later. Hence, according to the current rule, cohorts born later have to work up to two years longer before they are eligible to receive the full benefits than the cohorts born earlier.
Using data from the Health and Retirement Study (HRS) and the National Health Interview Survey (NHIS), Choi and Schoeni divided people born between 1933 and 1962 into four groups: those who are eligible to receive full retirement at age 65 (born 1933-1937), between 65 and 66 (born 1938-1942), at age 66 (born 1943-1954), between 66 and 67 (born 1955-1959), and at age 67 (born 1960-1962). They then examined several indicators of health conditions when each of these cohorts was at age 55-60. By comparing the health indicators at the same age across cohorts, they were able to show how health conditions have changed for each birth cohort in years leading to their respective retirement ages.
Choi and Schoeni found that, cohorts born more recently (and hence are only eligible to receive full Social Security benefit at ages higher than 65) are more likely to have limitations in their cognitive abilities and activities of daily living (ADL), as well as more likely to self-report as having fair or poor health, than the cohorts born earlier who can receive full benefit at age 65. When they split the sample by birth cohorts and levels of education, they also found that, holding the level of education constant, American workers who are eligible to receive full Social Security retirement benefit at later ages have higher morbidity of ADL limitations than those eligible to receive full benefit at age 65. The results regarding limitations in physical functioning and instrumental activities of daily living (IADL) are somewhat mixed; nevertheless, there is no evidence that the cohorts born later are in better health conditions than those born earlier.
Results reported by Choi and Schoeni are consistent with recent evidence that the health of near-elderly Americans has not improved in the past two decades. Given that people tend to claim retirement benefit at a later time as the full retirement age rises, the declining health conditions may lead to a higher share of workers in poor health conditions in the labor market. This would create challenges to employers and could potentially further destabilize the Social Security Disability Insurance (DI) program. Further increasing the full retirement age for the cohort approaching retirement may also cause substantial burden on these cohorts.
This article is published in Health Affairs:
HwaJung Choi and Robert F. Schoeni (2017). Health Of Americans Who Must Work Longer To Reach Social Security Retirement Age. Health Affairs, 36(10). https://doi.org/10.1377/hlthaff.2017.0217